eForm information
| Form ID | Form title | Who files | Where to file | When to file | Submittal options |
|---|---|---|---|---|---|
| RFA-1LC | Request for Further Action by Legal Counsel | Claimant's representative | Electronically filed with the Workers' Compensation Board, with PDF copy to employer's insurance carrier or directly to employer or third-party administrator if employer is a Board-approved self-insurer. | The form may be filed at any time after the assembly or indexing of a claim or after the Board has indicated that no further action (NFA) will be taken. |
|
Submitting via eCase
The new RFA-1LC retained the original three request categories (Compensation, Medical, and Other). Each category will have applicable request reasons that have been revamped for clarity and to obtain more details to ensure efficient processing.
Based on the request reason selected, the eForm will present guided questions and fillable sections required to submit the eForm.
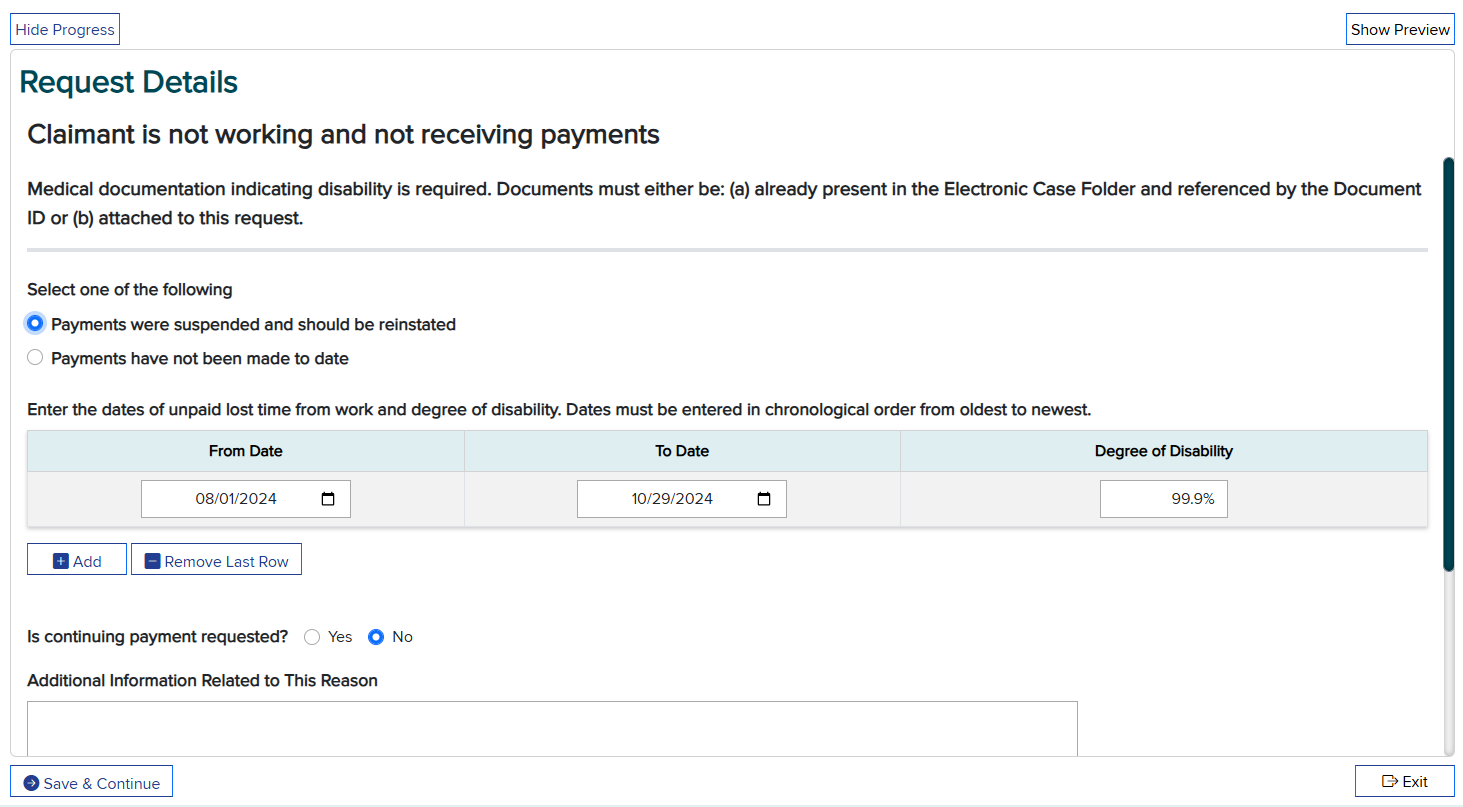
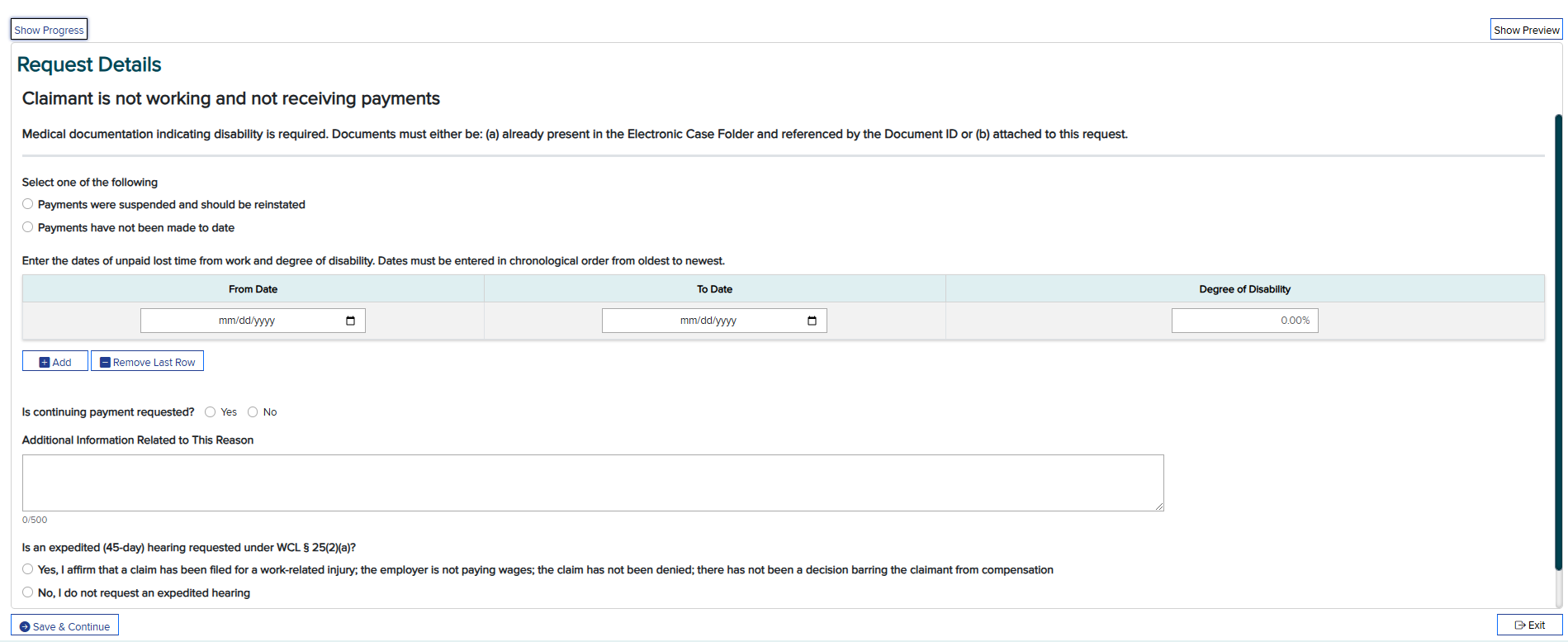
For example, questions for the request reason "Claimant is not working and not receiving payments":
- Select either "Payments were suspended and should be reinstated" or "Payments have not been made to date."
- Provide the From/To dates and the degree of disability.
- Answer Yes/No to "Is continuing payment requested?"
- Answer Yes/No to "Is an expedited (45-day) hearing requested under WCL (section symbol) 25(2)(a)?"
- Optional - a 500-character free form text box for additional information related to the request reason.
Once all questions and sections are complete, submit the eForm. See below for an in-depth breakdown of each step of the eForm.
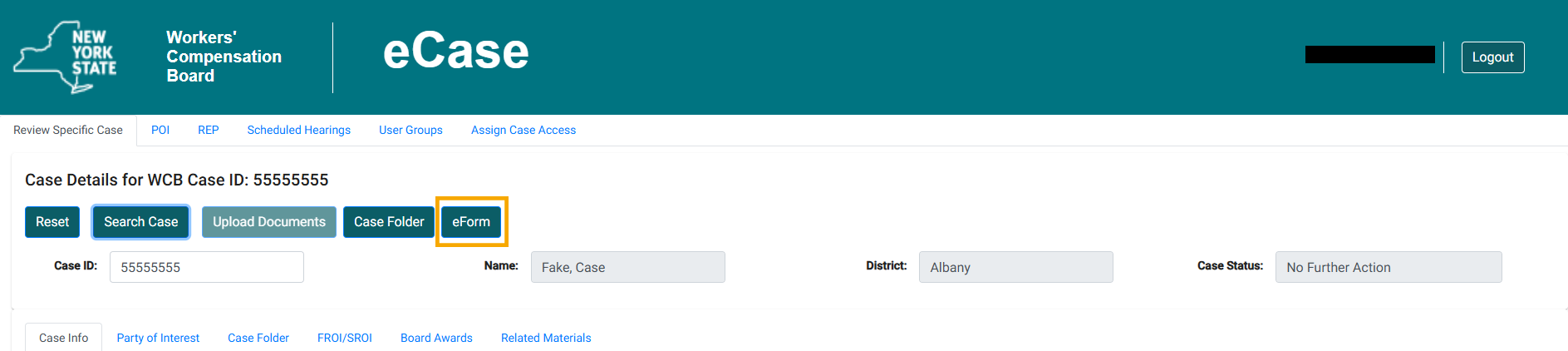
eForm button in eCase
Once logged into eCase, and a case number is entered, claimant attorneys and licensed representatives will see an eForm button.
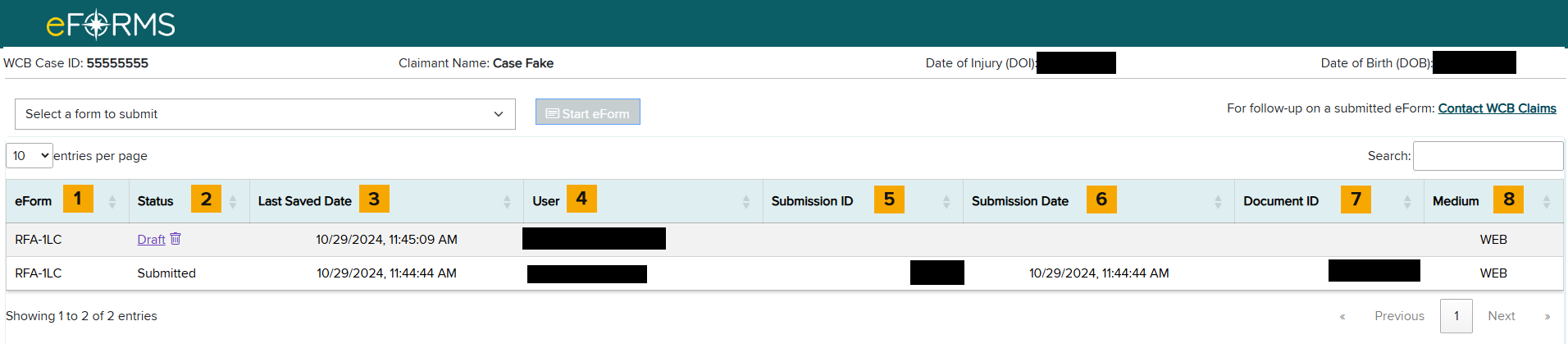
eForm landing page
After selecting the eForm button, you will be taken to the eForm landing page shown below.
From here, you can start a new eForm, as well as view all drafted and submitted eForms.
The landing page contains eight columns:
- eForm
- Status (eForm statuses are Submitted, Rejected, and Draft)
- Last Saved Date
- User
- Submission ID
- Submission Date
- Document ID
- Medium (Displays how the eForm was submitted - WEB, API, FTP)
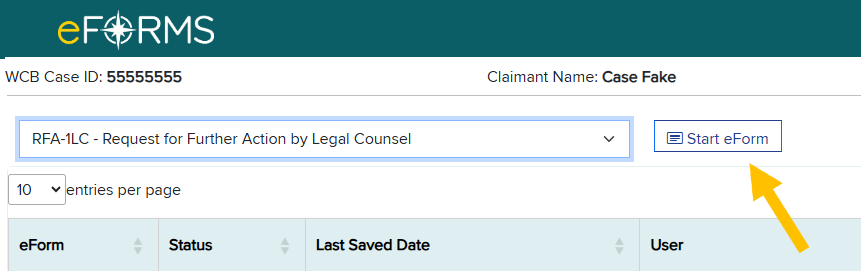
To start a new eForm, go to the Select a form to submit drop-down list and select RFA-1LC - Request for Further Action by Legal Counsel.
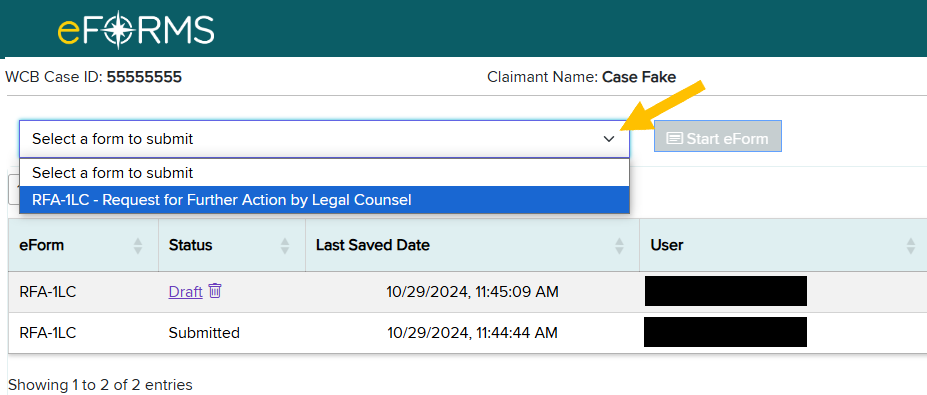
Then select the Start eForm button.
Selecting a request reason
Once a new RFA-1LC eForm is started, the page below will display on the screen. This page shows the request reasons. There are three categories of request reasons:
- Compensation
- Medical
- Other
Note: Some request reasons are conditionally displayed based on the type and state of the case at the time of submission.
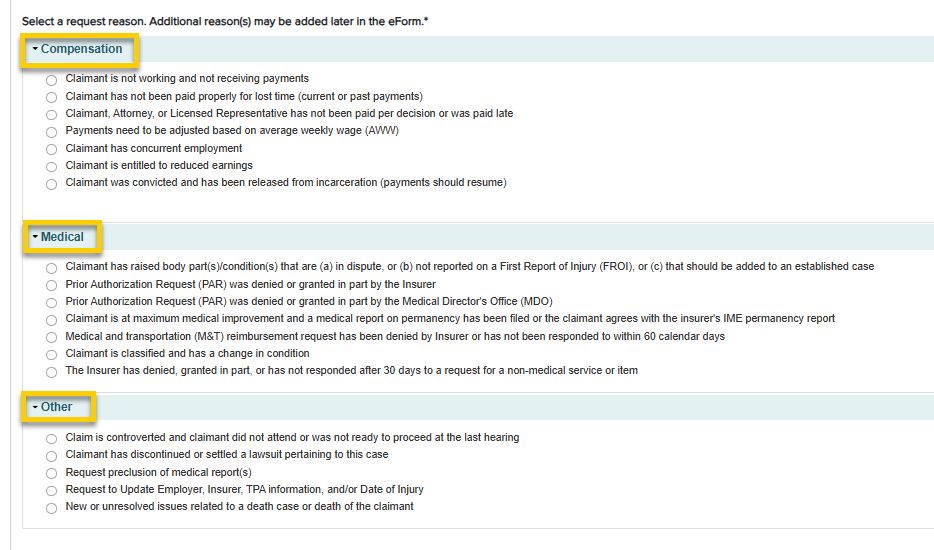
Select a request reason, and then click Save & Continue.
Completing the Request Details page
After selecting a request reason, you will be prompted to fill in the request details on the Request Details page. See Request Reason Quick Guide below for important information on request reasons.
| Request reason (RR) | Use for | Conditions for display | Requires certification | Link to resources | Reason abbreviation (API/XML) | RR medical provider name field value in eCase | Image example |
|---|---|---|---|---|---|---|---|
| Claimant is not working and not receiving payments |
Claimant needs payments re-instated Claimant has not received payments |
Will not display for volunteer firefighter/ambulance worker cases | Yes | Lost Wage Benefits | CNW | oow | |
| Volunteer firefighter/ambulance worker: Claimant is disabled and not receiving payments |
Claimant needs payments re-instated Claimant has not received payments |
Volunteer firefighter/ambulance worker case ONLY | Yes | Volunteer Firefighter Volunteer Ambulance |
CVW | oow | |
| Claimant has not been paid properly for lost time (current or past payments) |
Payments have been reduced Claimant has not been paid correctly in accordance with medical report/evidence Claimant is not working and not being paid property (i.e. carrier pays minimum, not in accordance with medical, etc.) Adjustment of prior payments (Claimant could be working or not working) |
Always displays | Yes | Lost Wage Benefits | CNP | lt | |
| Claimant, Attorney, or Licensed Representative has not been paid per decision or was paid late | Always displays | Yes | CAN | pen | |||
| Payments need to be adjusted based on average weekly wage (AWW) | Claimant has an issue with AWW for primary employer | Will not display for volunteer firefighter/ambulance worker cases | Yes | Calculating Your Average Weekly Wage | CAW | aww | |
| Claimant has concurrent employment | Employment in more than one job during the same time period | Will not display for volunteer firefighter/ambulance worker cases | Yes | Calculating Your Average Weekly Wage | CCE | cocn | |
| Claimant is entitled to reduced earning | A compensation rate based on the claimant's partial wage loss or partial loss of earning capacity due to a condition related to a compensable work-related injury. | Will not display for volunteer firefighter/ambulance worker cases | Yes | Lost Wage Benefits | CRE | re | |
| Claimant was convicted and has been released from incarceration (payments should resume) | Always displays | Yes | CRI | incar |
| Request reason (RR) | Use for | Conditions for display | Requires certification | Link to resources | Reason abbreviation (API/XML) | RR medical provider name field value in eCase | Image example |
|---|---|---|---|---|---|---|---|
| Claimant has raised body part(s)/condition(s) that are (a) in dispute, or (b) not reported on a First Report of Injury (FROI), or (c) that should be added to an established case | Claimant needs to establish additional body parts that are not accepted/established Body part has been disputed Body part raised in a decision and not resolved Request to accept body part was sent to claim administrator without response |
Always displays | Yes | Workers' Compensation Health Care | MBC | ancr | |
| Prior Authorization Request (PAR) was denied or granted in part by the Insurer | Requesting review of a PAR. Only PARs that are eligible for review are displayed for selection. | Always displays | No | What is a Prior Authorization Request? | MPI | par | |
| Prior Authorization Request (PAR) was denied or granted n part by the Medical Director's Office (MDO) | Requesting review of a NOR that ruled on a PAR. Only NORs that are eligible for review are displayed for selection. | Always displays | No | What is a Prior Authorization Request? | MPM | mdo | |
| Claimant is at maximum medical improvement and a medical report on permanency has been filed or the claimant agrees with the insurer's IME permanency report | Claimant is in agreement with the Insurer's IME report on permanency A medical report on permanency has been filed Doctor's Report of MMI/Permanent Impairment (Form C-4.3) and Notice Regarding Possible Award for Permanent Injury (SLU or Facial)(EC-81.7) |
Always displays | No | Awards for Loss of Use or Permanent Disability | MCI | mmi | |
| Medical and transportation (M&T) reimbursement request has been denied by Insurer or has not been responded to within 60 calendar days | Medical and transportation reimbursement has been denied Medical and transportation reimbursement has been submitted to the Insurer and more than 60 days has elapsed without response |
Always displays | Yes | Health Care Factsheet Claimant Information Packet |
MTR | m&t | |
| Claimant is classified and has a change in condition | Claimant classified permanent partial disability (PPD) - overall reclassification (C-4.3) - asking for reclassification but do not file C-4.3, user can't proceed with request -Temporary Total Disability (TTD) benefits - not as a result of surgery, file an RB-89 |
Always displays | Yes | MCC | ppd or reclass | ||
| The Insurer has denied, granted in part, or has not responded after 30 days to a request for a non-medical service or item | Claimant's doctor prescribes a non-medical service or item that cannot be submitted through the PAR process. | Always displays | Yes | MAN | auth |
| Request reason (RR) | Use for | Conditions for display | Requires certification | Link to resources | Reason abbreviation (API/XML) | RR medical provider name field value in eCase | Image example |
|---|---|---|---|---|---|---|---|
| Claim is controverted and claimant did not attend or was not ready to proceed at the last hearing | Will display ONLY if the case is NOT established and there are past hearings present in the system | No | Glossary description: A workers' compensation claim that is disputed by the employer or by the employer's insurer. Each side presents its case at a hearing and a judge then makes a decision. | OCC | ftp | ||
| Claimant has discontinued or settled a lawsuit pertaining to this case | Always displays | Yes | Glossary description: Lawsuits against equipment manufacturers, facility owners and other non-employer parties whose products or services contributed to the occurrence of an accident. Under the Workers' Compensation Law, a compensation claim is a worker's sole remedy against the employer, but lawsuits may be initiated against third parties for contributory negligence, product defects, etc. | OCD | 3pa | ||
| Request preclusion of medical report(s) | Insurer did not comply with Section 137 requirements for the IME | Always displays | Yes | ORP | 137 | ||
| Request to Update Employer, Insurer, TPA information, and/or Date of Injury | Wrong employer/insurer/TPA is on notice An additional employer, carrier or TPA should be placed on notice Correction is required for current employer/insurer/TPA No Fault Insurer needs to be placed on notice |
Always displays | No | OEI | poi | ||
| New or unresolved issues related to a death case or death of the claimant | Further action requested on a death case Spouse remarries Beneficiary cannot be located Beneficiary has passed away Marriage is annulled Beneficiary reaches 18, 23, or 25 (25 only applicable to Volunteer Ambulance and Volunteer Fire cases) Beneficiary is no longer a student Beneficiary is a student Beneficiary is declared adult dependent Beneficiary is dependent Beneficiary is no longer a dependent |
Always displays | No | Death Claims | OUI | death | |
| Additional Proposed Findings | Use For | Conditions for Display | Requires Certification | Link to Resources | Abbreviation (API/XML) | Medical Provider Name field value in eCase | Image Example |
| Establish case (ANCR/ODNCR) as accepted on a First Report of Injury (FROI) Establish average weekly wage (AWW) Award lost wage benefits as per Subsequent Report of Injury (SROI) Attorney or Licensed Representative fee requested |
Always displays | Yes | Not applicable | pf |
In the example below, the request reason "Claimant is not working and not receiving payments" will require you fill in the payment and lost time information and whether an expedited hearing is requested. Select Save & Continue when you are finished.
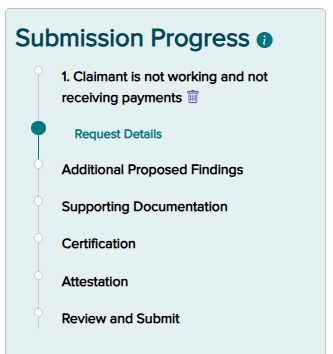
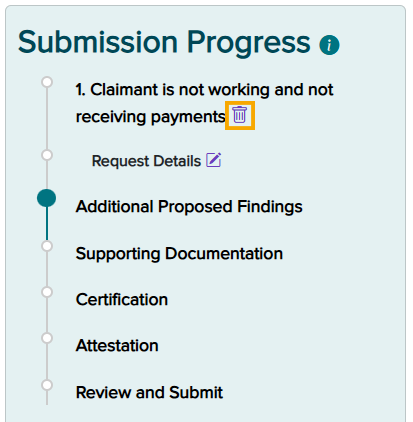
Submission Progress panel
The Submission Progress panel allows you to keep track of the eForm's progress as you complete each step.
Saving a draft
You can save a draft or exit at any point while filling out the eForm. When you select Exit, the message window below displays on the screen. If you select "Confirm," you are acknowledging that the progress on the current step you are on will be lost and a draft with all previously completed information will be saved.

Adding another request reason
Multiple reasons can be submitted on an RFA-1LC eForm. You may add another request reason once the first request reason has been completed. After saving the request details, a prompt will appear asking if you want to add another request reason. Select Yes to add an additional request reason.

Editing a request reason
To edit request details, select the pencil icon shown on the Submission Progress panel.
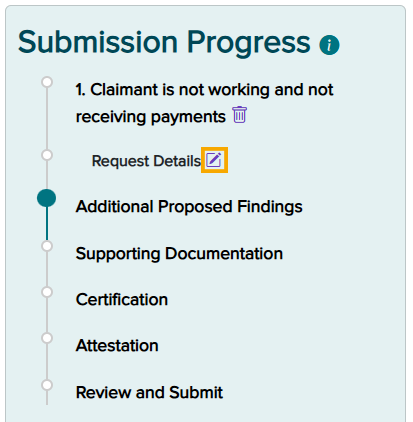
Note: You must click the Save & Continue button in order for the pencil icon to appear next to a step in the eForm.
Deleting a request reason
If a request reason was selected in error, select the trash can icon displayed in the Submission Progress panel. This will delete the request reason and return you to the list of reasons.
Upon selecting this icon, you will be prompted to confirm deletion of the record.
Select Delete.
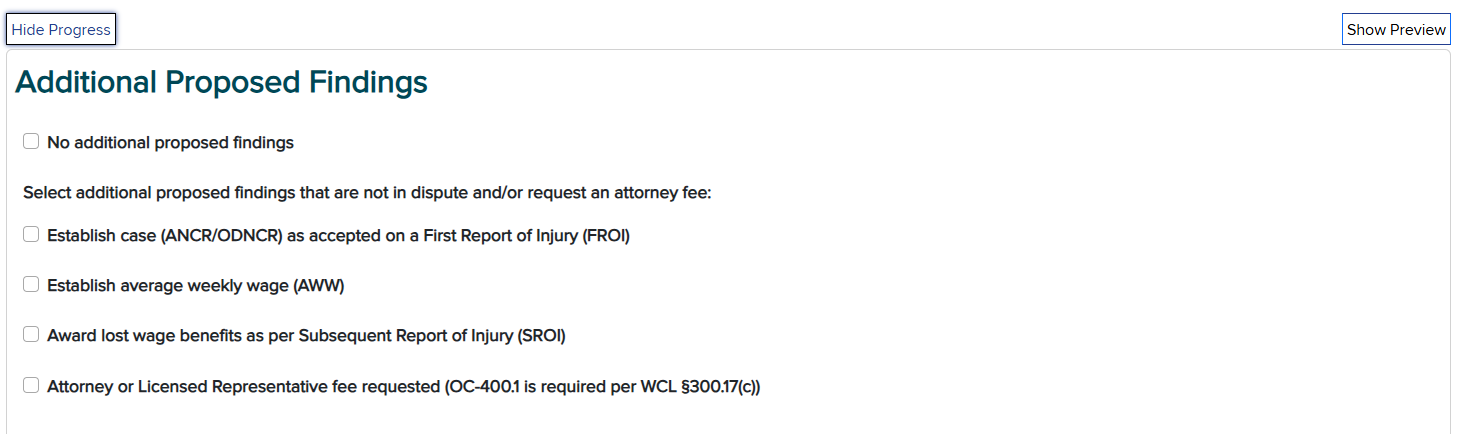
Additional Proposed Findings page
The Additional Proposed Findings page allows you to add findings that are not in dispute and/or request an attorney fee. Choose from the following:
- Establish case (ANCR/ODNCR) as accepted on a First Report of Injury (FROI)
- Establish average weekly wage (AWW)
- Award lost wage benefits as per Subsequent Report of Injury (SROI)
- Attorney or Licensed Representative fee requested (OC-400.1 is required per WCL §300.17(c))
Otherwise, select the No additional proposed findings check box.
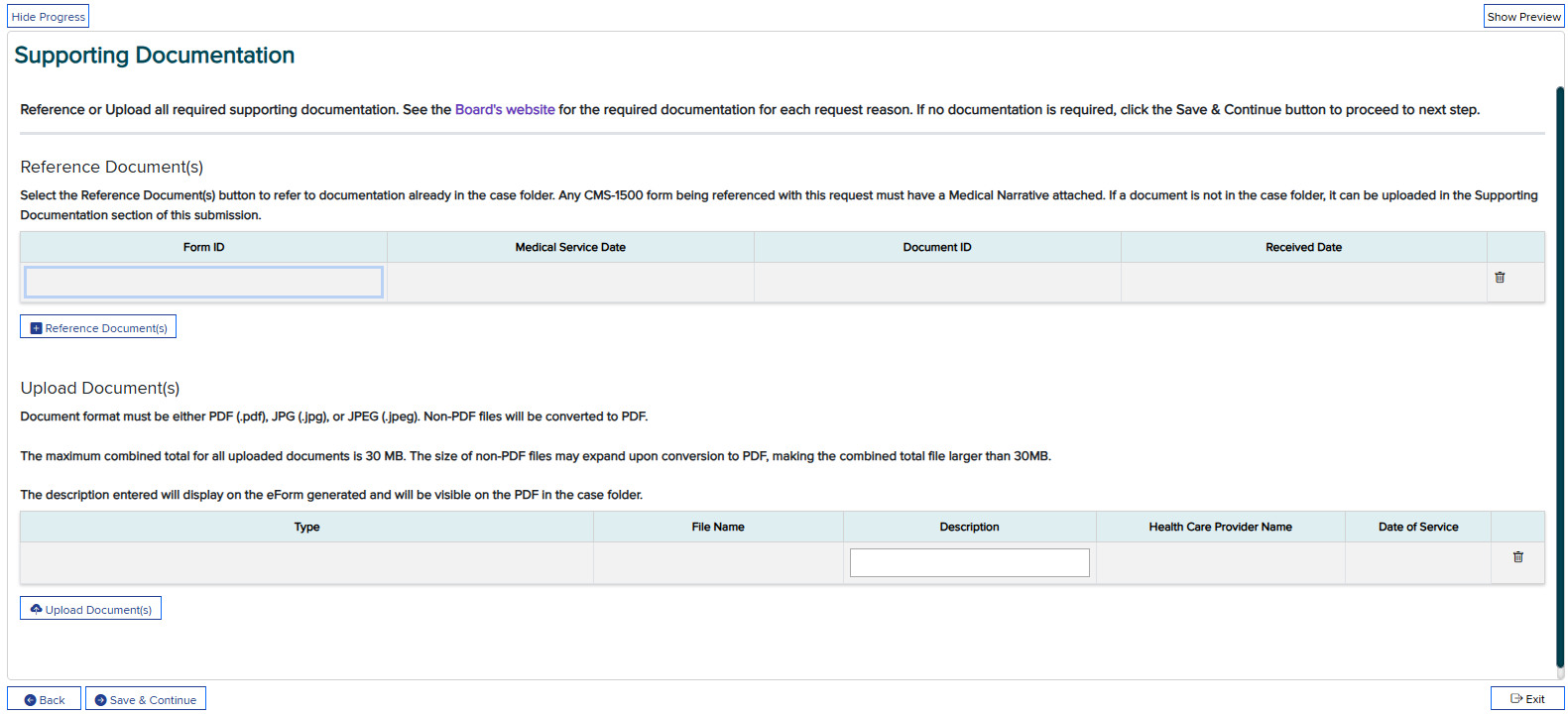
Supporting Documentation page
The Supporting Documentation page allows you to reference documents from the case folder or upload supporting documentation for the eForm. Please refer to the Required Document Matrix (MS Excel) for more information on required documentation.
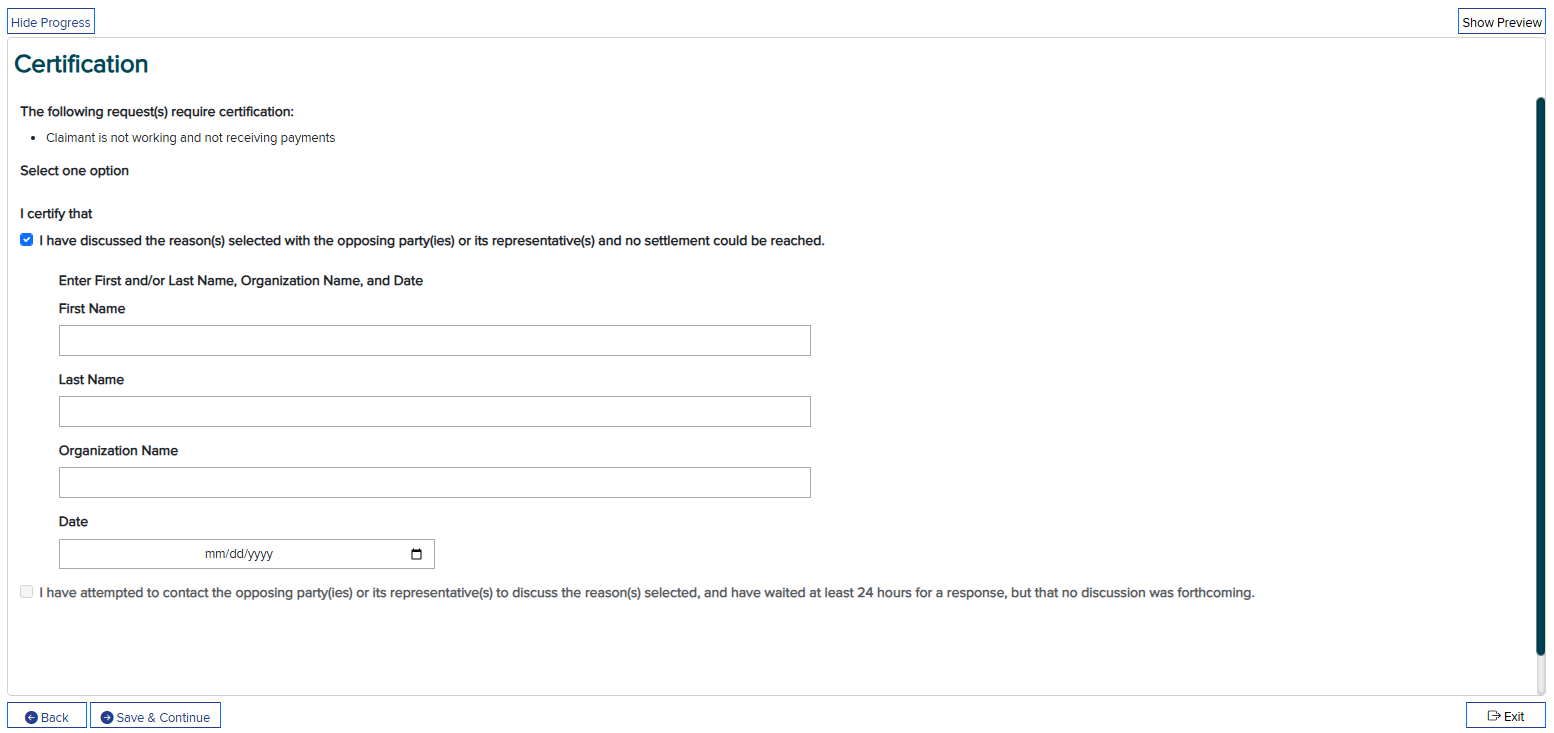
Certification page
Certification may be required for a request reason/additional proposed findings if there was a FROI/SROI submitted on behalf of the primary insurer for the WCB Case ID. It is the responsibility of the claimant's attorney or licensed representative to serve all parties, including any official Board forms uploaded with the eForm submission.
Note: The certification date cannot be the current date.
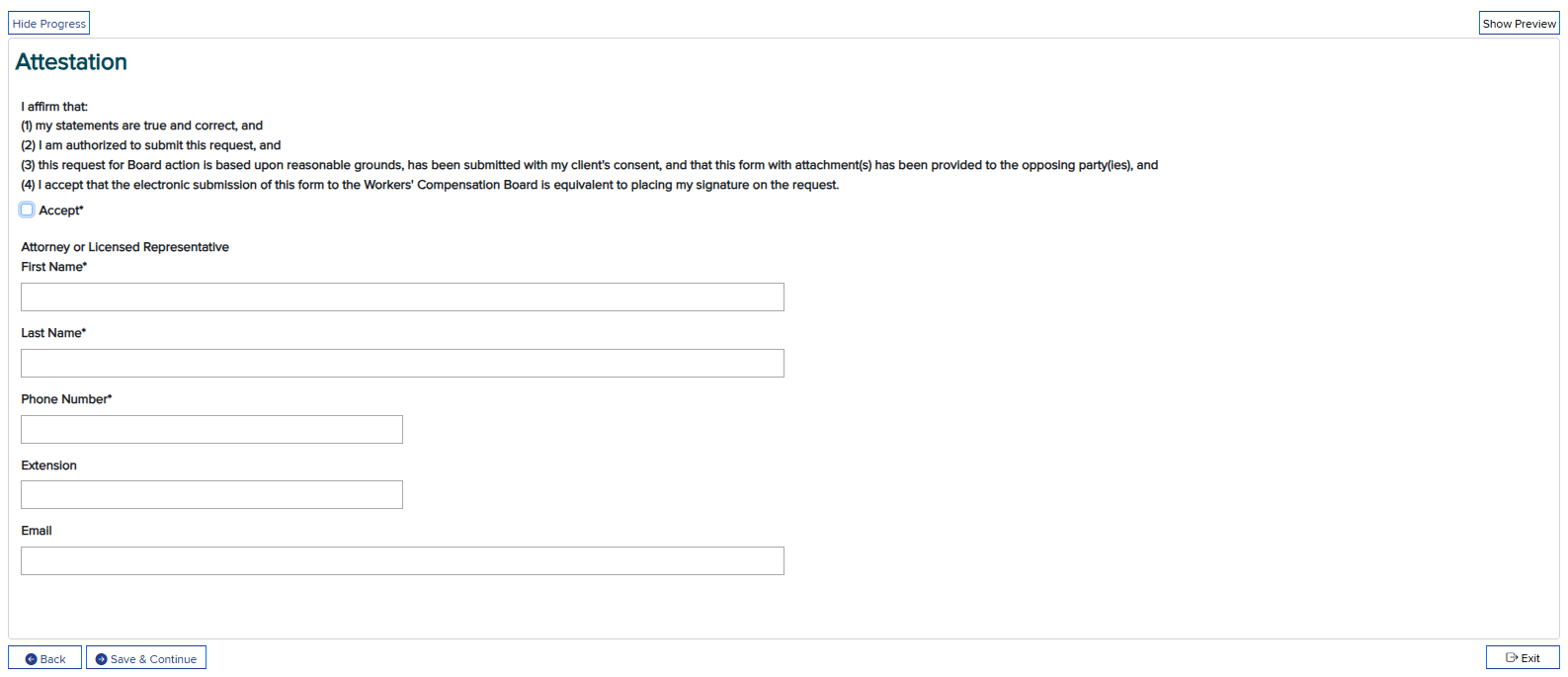
Attestation page
To submit the eForm, you must accept the Attestation.
Note: The First Name, Last Name, and Organization Name fields should be the information of the attorney or licensed representative assigned to the case, not necessarily the person submitting the form. The Attestation text is shown below.
I affirm that:
(1) my statements are true and correct, and
(2) I am authorized to submit this request, and
(3) this request for Board action is based upon reasonable grounds, has been submitted with my client's consent, and that this form with attachment(s) has been provided to the opposing party(ies), and
(4) I accept that the electronic submission of this form to the Workers' Compensation Board is equivalent to placing my signature on the request.
Fill in the attorney/representative information, and then select the Accept check box. Click Save & Continue when you are finished.
Review and Submit page
Prior to submitting the eForm, you will have a chance to review a draft of your submission. Click the Back button to edit the eForm or delete a request reason.
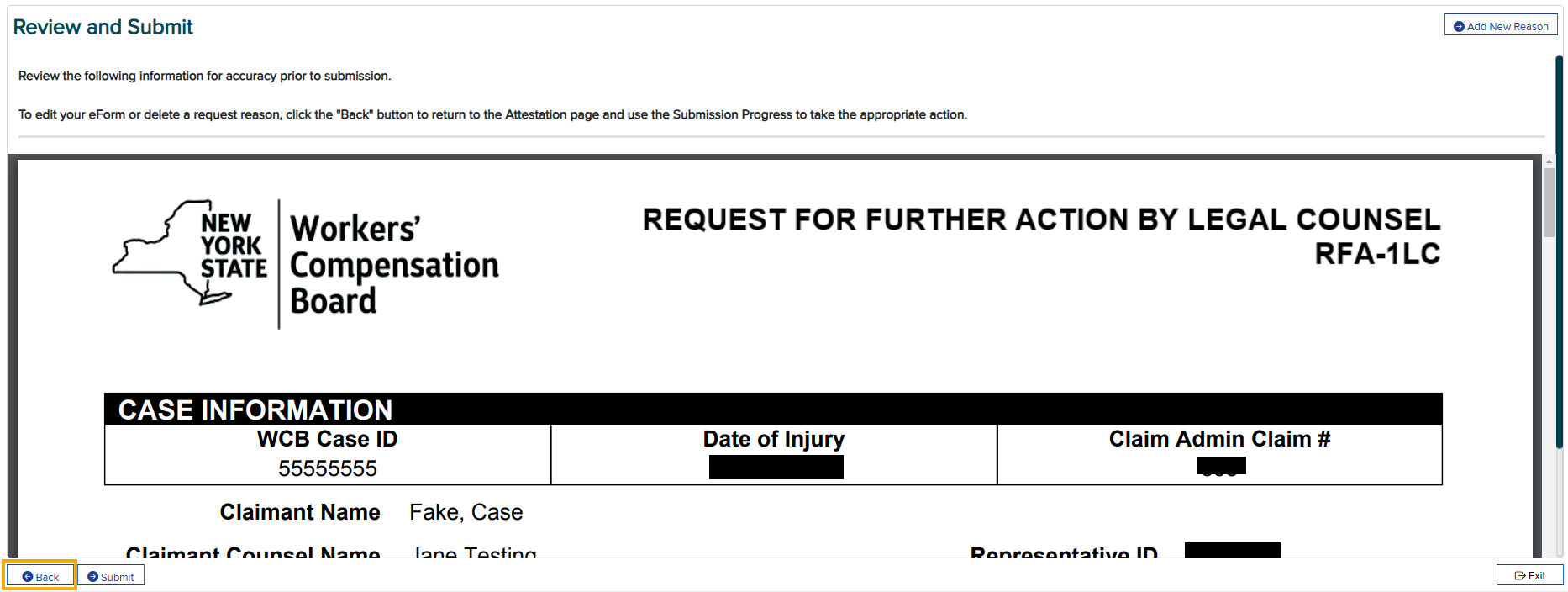
Upon submission, the system automatically generates a PDF and places it in the case folder. You will be able to view/print/download the PDF from the eForms landing page and via eCase. You can also view submitted eForm details, including submitted status, on the eForms landing page.
Submitting via API or XML file
- Registration Instructions
- Testing Requirements for API Submission
- Testing Requirements for XML File Submission
Requirements and examples
| File name | Description |
|---|---|
| RFA-1LC-XML-Data-Requirements-and-Edits.xlsx | XML documentation/guidelines for RFA-1LC XML data elements. This spreadsheet contains list of error codes, list of valid values, element requirements and element rules. |
| eFormsCnw1.xml | XML layout example for RFA-1LC submission of request reason code CNW (Claimant is not working and not receiving payments) |
| eFormsCaw1.xml | XML layout example for RFA-1LC submission of request reason code CAW (Payments need to be adjusted based on average weekly wage (AWW)) |
| eFormsCvw1.xml | XML layout example for RFA-1LC submission of request reason code CVW (Volunteer firefighter/ambulance worker: Claimant is disabled and not receiving payments) |
| eFormsMbc.xml | XML layout example for RFA-1LC submission of request reason code MBC (Claimant has raised body part(s)/condition(s) that are (a) in dispute, or (b) not reported on a First Report of Injury (FROI), or (c) that should be added to an established case) |
| eFormsMci1.xml | XML layout example for RFA-1LC submission of request reason code MCI (Claimant is at maximum medical improvement and a medical report on permanency has been filed or the claimant agrees with the insurer's IME permanency report) |
| eFormsXMLAckTemplate.xml | XML acknowledgement template for RFA-1LC. After processing the API submission the acceptance and rejection of the transaction will be returned back to the sender. |
| eFormsXmlTemplate.xml | XML template for the RFA-1LC submission. This template contains the data elements for all submission reasons. It is recommended to review the API requirements and edits spreadsheet for the submission reason specific data element list. |
| eFormsRfa1lc.xsd | XML schema definition for RFA-1LC XML data submission. API submitters are expected to use this schema definition to validate the data before sending XML submission via API. |
| Required-Document-Matrix.xlsx | This document will assist you in determining if supporting documentation will be needed (referenced or submitted) when submitting the RFA-1LC. |
| Submitted-RFA-1LC-sample-1.pdf | This is a sample of a generated RFA-1LC after it was submitted to the Board when a claimant is not working and is not receiving payments at this time. |
| Submitted-RFA-1LC-sample-2.pdf | This is a sample of a generated RFA-1LC where there are multiple reasons for the form submission. |
| Submitted-RFA-1LC-sample-3.pdf | This is a sample of a generated RFA-1LC where the payor has denied or partially granted a Prior Authorization Request (PAR) from a medical provider treating the claimant. |
FAQs
-
Will the eForm option automatically be available beginning December 13, 2024, or is there a separate step that an eCase user may need to take to ensure they have this access?
It will automatically be available on December 13. Users will need to perform a successful case search before the eForm button appears.
-
Is there an opt-out option (e.g., submitting by U.S. mail)?
No, you must submit electronically starting on December 13, 2024. After this date, the Board will not accept or act on any paper RFA-1LC forms submitted by attorneys/representatives.
-
Will we still have a testing environment for API after December 13, 2024?
Yes. We encourage firms that have an interest in pursuing our XML options to visit the RFA-1LC eForm page. Testing for both the API and the sFTP file-based options will continue to be available after December 13.
-
Is there an option to download the completed RFA-1LC eForm?
Yes, you can download or print a PDF of the completed eForm. Submitted eForms are placed in the case folder and can be viewed from the eForms landing page using the Submission ID hyperlink. The hyperlink will open the PDF.
-
Does a copy of the eForm automatically get sent to the required parties (e.g., insurer, claimant)?
A copy of the completed RFA-1LC eForm is not automatically sent to the required parties. It is the responsibility of the claimant's legal counsel to download and print the completed eForms and serve all parties the RFA-1LC and any uploaded documents following the same methods currently being used to serve all parties.
-
Is there any way to fix mistakes on the RFA-1LC eForm after it is submitted?
No, once the RFA-1LC is submitted, no other changes can be made. However, the form can be saved and edited as a work in progress before submission.
-
If an attorney chooses to withdraw an RFA-1LC that was submitted, how do they do that?
You cannot cancel the RFA once it's been submitted, but you can send attorney correspondence to the Board and parties of interest stating that you withdraw the RFA-1LC that was filed.
-
Can supporting documentation be attached after the RFA-1LC is filed?
No, submit the documentation with attorney correspondence if you need to reference additional documentation in relation to the RFA-1LC.
-
Is supporting documentation required for every RFA-1LC submission?
Use the Required Document Matrix file from the Requirements and examples section above to assist you in determining if supporting documentation will be needed (referenced or uploaded).
-
Can multiple users at the same law firm access and update eForm drafts on the landing page?
There can only be one draft per WCB case number. Only one person can work in a WCB case number at a time. One user can start an eForm, save a draft, and another user can resume that draft and save or submit it.
-
Will there be a different way to upload attorney fee applications?
If an attorney fee is being requested in relation to the issue raised on the RFA-1LC, select the option "Attorney or Licensed Representative fee requested" under the Additional Proposed Findings step and upload/reference your Application for Fee by Claimant's Attorney or Licensed Representative (Form OC-400.1) with the eForm submission.
As a reminder, per our Efficiency Enhancements GovDelivery , do not use eCase Upload to submit your OC-400.1 after the hearing is closed. OC-400.1 form submissions trigger automatic Board action without additional correspondence but will not do so if instantly uploaded after the hearing has closed.
OC-400.1 follow-up may be requested by submitting an online claims inquiry and selecting "Request Board action on case documents."
-
When we file an RFA-1LC for a Section 32 agreement or stipulation, do we just attach the agreement and all necessary papers along with the RFA?
No, do not file an RFA-1LC. The Section 32 agreement or stipulation creates a work item for the examiner to review. If these actions do not automatically happen within 30 days, you can submit an online claims inquiry.
-
Can the RFA-1LC be used for Level 3 PAR denials?
Yes, under the Medical Category, select "Prior Authorization Request (PAR) was denied or granted in part by the Medical Director's Office (MDO)." You will be required to reference the appropriate PAR(s). PAR(s) eligible for selection have the following Form IDs: MG2-L3D, RX-L3D, DME-L3D, SS-L3D, MG2-L3GP, RX-L3GP, DME-L3GP, SS-L3GP.
If a specific PAR document does not appear, please refer to the "PAR Denial Appeals" section on Board's website for a list of PAR denial types the attorney may request for Adjudication review.
-
Can I request review of a PAR using the request reason of "Insurer has denied, granted in part, or has not responded after 30 days to a request for a non-medical service or item"?
No, you cannot use this reason for medical authorization requests that have been submitted by the claimant's health care provider through the Prior Authorization Request (PAR) process. PARs that are eligible for Adjudication review will appear as a document to select within these two request reasons: "Prior Authorization Request (PAR) was denied or granted in part by the Insurer" and "Prior Authorization Request (PAR) was denied or granted in part by the Medical Director's Office (MDO)." If a specific PAR document does not appear, please refer to the "PAR Denial Appeals" section on the Board's website for a list of PAR denial types the attorney may request for Adjudication review.
-
How do I request a Notice Regarding Possible Award for Permanent Injury, Schedule Loss of Use, or Facial (Form EC-81.7)?
To request that the Board act on a permanency report, file an RFA-1LC using the request reason "Claimant is at maximum medical improvement and a medical report on permanency has been filed or the claimant agrees with the insurer's IME permanency report."
-
How do you request a hearing for facial disfigurement?
To request that the Board act on a permanency report, file an RFA-1LC using the request reason "Claimant is at maximum medical improvement and a medical report on permanency has been filed or the claimant agrees with the insurer's IME permanency report."
Attorney correspondence can be uploaded with the RFA-1LC if an in-person hearing is requested for facial disfigurement.
-
How do I request to cross-examine on the issue of permanency using the RFA-1LC eForm?
Do NOT file an RFA-1LC using the request reason "Preclusion of Medical Reports" for this issue.
First, consider if you have already filed an RFA-1LC using the request reason "Claimant is at maximum medical improvement and a medical report on permanency has been filed or the claimant agrees with the insurer's IME permanency report." If not, then you should file one to request Board action on a permanency report.
If an EC-81.7 has been issued for schedule loss of use, then depositions will be directed automatically by Proposed Decision without any further action required by the parties. For permanency reports noting non-schedulable injuries, a hearing will be scheduled when the RFA-1LC is filed. If these actions do not happen within 30 days, you can submit an online claims inquiry.
For other topics where cross-examination is desired, select the appropriate request reason related to the joined issue on the RFA-1LC and indicate in the additional information field that you are requesting depositions/testimony. If the request reason is not on RFA-1LC, submit attorney correspondence.
-
How do I request to expedite claims for additional sites of injury and consequential injuries?
When the Board receives an RFA-1LC presenting prima facie medical evidence (PFME) for an unestablished injury or condition, the Board will issue a Proposed Decision finding PFME, and will afford the insurer the right to accept the condition, get an independent medical examination (IME), cross-examine the health care provider, or make an argument on the record.
Once the Board issues the PFME Proposed Decision, it will set the case for a hearing approximately 75 days later. At that hearing, the insurer must produce the evidence directed by the Proposed Decision. In addition, the parties will have the opportunity to take brief testimony of the claimant on mechanism of injury. If an IME does not contest the injury or condition, the judge will make a decision on the additional site at this first hearing.
If the IME finds that the injury is not related, and depositions are requested, the judge will grant a continuance for outcome of those depositions. It is expected, absent good cause, that the Board will resolve these issues within one to two hearings.
Note: A Claimant's Notice of Independent Medical Examination (Form IME-5) or proof of a testimony date must be in the file by the date the Proposed Decision becomes final, or the Board may deem the insurer's inaction as a waiver of the right to get an IME or cross-examine claimant's provider. In addition, to be considered timely, any requests for a broader release of medical records should be made well in advance of the scheduled hearing.
-
How do I alert the Board that a case is ready for a decision?
In schedule loss of use cases when an EC-81.7 has been issued or where a judge has continued a case for a hearing or Reserved Decision, there should be follow-up action already scheduled by the Board. No RFA-1LC is necessary.
For other topics where the Board has directed the parties to follow-up, do one of the following:
- Submit an online claims inquiry and select "Request Board action on case documents."
- Select the appropriate request reason related to the joined issue on the RFA-1LC and indicate in the additional information field that you are requesting depositions/testimony.
- If the request reason is not on RFA-1LC, then submit attorney correspondence.
-
How do I submit for something not included on the RFA-1LC eForm?
First, consider whether the Board needs a request on that topic. For example, any of the following will trigger Claims action without the need for an RFA-1LC or attorney correspondence: Section 32 waiver agreement, Stipulation (Form C-300.5), and Agreed Upon Proposed Decision Findings (Form C-312.5). Sending unnecessary requests will cause delays.
For issues that do not result in an automated Board action, the attorney may submit attorney correspondence. Do NOT file an RFA-1LC using a request reason that does not apply.
-
Where is the spot for the free text?
The free text option is within the Request Details step (if available for that request reason).
-
How can I attach evidence?
On the RFA-1LC eForm, select the appropriate request reason. Documents can be selected from the case file or uploaded from the user's device within that request reason.
-
How can I raise reattachment to the labor market?
If the claimant alleges they have reattached to the labor market and payments should resume, then select request reason "Claimant is not working and not receiving payments," upload the attachment evidence, and write "Claimant has reattached to the labor market" in the Additional Information Related to This Reason free text field.
-
How can I check the status of a previously submitted RFA-1LC?
If required, status on a previously submitted RFA-1LC may be checked by submitting an online claims inquiry and selecting "Request for Further Action (Form RFA-1LC) status." Please give the Board at least 30 days before submitting an inquiry.
-
How does the attorney request a hearing per a WCB Board Panel decision?
If there is a direction in the WCB Board Panel decision to have a hearing, the case will be scheduled automatically; no RFA-1LC is needed. Follow-up may be requested by submitting an online claims inquiry and selecting "Request Board action on case documents."
If there isn't a direction for further hearings, then select a reason on the RFA-1LC eForm that needs to be addressed or submit attorney correspondence.
-
How can I update a claimant's information?
Notify the claim administrator of the change and copy the Board. If there isn't a claim administrator on file, send the information to the Board.
-
How do I indicate an interpreter is needed?
If an interpreter is needed for a hearing, ensure an Employee Claim (Form C-3) is filed indicating that an interpreter is required. More information is also available in the Claimant Information Packet.
-
How do I request action if the Claim Administrator has improperly granted a PAR without prejudice for a site/condition that has been accepted or established?
Submit attorney correspondence raising the issue that the Claim Administrator improperly used Granted Without Prejudice for an accepted or established site/condition and identify the document ID number of the PAR. Do NOT file an RFA-1LC using a request reason that does not apply.
More information
Need help or have feedback? Email OnBoard@wcb.ny.gov. Please include the following in your correspondence, where applicable:
- User ID
- R#
- Request reason(s)
- Field or XML data element name
- Details of issue
- Screen shot
Additional resources
RFA-1LC eForm training webinar
RFA 1LC Attorney Engagement Sessions April 2023
Technical support
For technical assistance, please email WCBTechnicalSupport@wcb.ny.gov.